Women in northwestern Syria pay the price of donor fatigue
Eleven years on, funding for Syria is stagnating while needs grow. Women are among those most affected by funding gaps in the health sector.
12 May 2022

PARIS — In parts of Syria, the impact of donor fatigue and funding gaps can be fatal, and women are disproportionately affected. In northwestern Syria, “there’s a shortage of pretty much everything—supplies, medicine, but also qualified staff,” Osama*, a doctor managing medical activities in northwest Syria for the humanitarian NGO Doctors Without Borders (MSF), told Syria Direct.
Osama recalled one recent case of a young patient infected with COVID-19 near the end of her pregnancy. “She needed to be in an intensive care unit as well as to receive an operation that is difficult to have throughout the region. Moving her from the ICU of one hospital to another hospital to perform a cesarean section in order to save her child was very challenging, and unfortunately the patient did not survive,” he said.
The tragedy could have been avoided, Osama said, if either hospital had been equipped with an ICU and the equipment necessary to carry out a C-section—a common operation that accounts for one in five childbirths worldwide according to the World Health Organization.
Unfortunately, the vast majority of health facilities in northwest Syria currently lack adequate funding, equipment and staff—and for a number of cultural, social and economic reasons, women are on the frontline of this health crisis.
Dwindling funding
Years of war have devastated Syria’s health system, once one of the best in the region, and left the country precipitously low on medical staff.
Syrian hospitals and first aid responders have been systematically targeted in recent years. At least 942 medical staff were killed in Syria between March 2011 to March 2022, according to Physicians for Human Rights, which documented more than 600 attacks against 400 healthcare facilities over the same period. The vast majority of the attacks (542) were attributed to the regime and its ally Russia. Beset from all sides, many medical workers emigrated: an estimated 70 percent of Syrian health workers left the country as of March 2021, leaving just one doctor for every 10,000 Syrians.
“After more than a decade of conflict, the health system [in northwest Syria] is completely reliant on international NGO funds,” Osama stressed. International aid has become a lifeline, particularly in the northwest—the last opposition-held region, home to 4.4 million people, including 2.8 million displaced by the war.
Supported by international donors, international medical organizations and their local partners have stepped in to substitute the public health system. But this precarious flow of money threatens to run dry. Human rights watchdog Amnesty International warned earlier this week of a “severe health crisis” in the northwest, where funding for the health sector has dropped by more than 40 percent over the past ten months.
Part of the lost funding is due to decreasing donor interest in Syria, a trend donors themselves recognize. “I know there is a certain fatigue. How not, after eleven years of conflict,” Josep Borrell, the European Union’s High Representative for Foreign Affairs and Security Policy, told EU ministers on May 9, the opening day of the Brussels VI conference—an annual event during which European states announce their funding pledges for Syria.
“The world’s public opinion seems not to be able to deal with more than one crisis at a time. Now, there is Ukraine on the headlines, but do not give up on Syria,” Borrell added, echoing the concerns of humanitarian actors who have warned that Russia’s invasion of Ukraine could detract attention from other crises, and divert essential humanitarian funding.
The Brussels VI conference concluded on May 10 with $4.3 billion pledged for 2022, on top of $2 billion pledged last year “for 2022 and beyond”). The funding is in line with 2021 amounts ($6.4 billion) but falls short of the $10.5 billion sought by the UN for 2022. It is also expected to have limited impact, due to rising humanitarian needs and skyrocketing food prices exacerbated by the war in Ukraine. Earlier this month, the UN World Food Programme had to reduce food assistance to the region due to budget cuts.
It’s not just funding cuts: the fate of cross-border aid to Syria through Bab al-Hawa, northwest Syria’s largest humanitarian crossing, will hang in the balance in July. UN convoys can only use this crossing if the UN Security Council, on which Russia sits, renews a yearly resolution authorizing them to do so. If Russia vetoes the resolution and the crossing closes, all humanitarian activities in the region will be heavily affected.
Severe shortages, skyrocketing costs
Even as funding decreases, needs keep growing in northwest Syria, which is in the midst of a severe humanitarian crisis compounded by the COVID-19 pandemic. Less than five percent of the population there is fully vaccinated.
Women in Idlib province who spoke to Syria Direct all mentioned the skyrocketing cost of healthcare, which they say “doubled” over the past year. “On average, the cost of a visit to the doctor is equivalent to a worker’s full day’s wage,” Fatima al-Shahoud, a nurse in a public hospital in Idlib, added. “Today, an examination [in a private hospital] costs no less than the equivalent of 40 Turkish lira.”
“The price of medicines, equipment and all medical supplies—even non-medical things like food, fuel, electricity—has been increasing exponentially in the past year and in 2022,” Osama added. This is largely due to the collapse of the Turkish lira, which lost 44 percent of its value in 2021, driving up the price of imported products. Turkish lira are used in this border area in lieu of Syrian pounds, whose value plummeted during the war.
To manage rising costs and budget cuts, hospitals have had to roll back some services and limit the medicine they provide for free. Health officials in Idlib province say 10 out of 50 hospitals, including six gynecology and pediatric hospitals, lost funding and closed in 2022, and more could close soon.
“Where I live, there is no health center or hospital providing women’s health services within a 20-km radius,” Zubaida*, a midwife with MSF, told Syria Direct. The paucity of doctors is felt across all hospitals—public and private, in major cities like Idlib, and especially in rural areas.
Shortages in medical staff particularly affect women, who often require specialized medical care during pregnancy. “It’s challenging to find qualified medical staff in general, but especially specialists, and particularly female gynecologists,” Osama pointed out. “Because of cultural aspects, patients will almost always want to see a female health practitioner, which adds another layer of complexity.” To fill this gap, the NGO system is “trying to adapt to the shortage of specialists by focusing more on providing primary healthcare through midwives,” Osama added.
Midwives are the “cornerstone” of sexual, reproductive and maternal health, Osama stressed. They typically monitor and assist pregnancies, manage vaginal deliveries, and provide family planning services and advice. And in many countries in crisis, including Syria, their role is expanding.
“Midwives have started to get training to manage more high-risk pregnancies,” Zubaida said. “Those working in emergency rooms must be able to provide certain services, whether there is a doctor present or not. The experience and qualifications of midwives have increased in general, and most organizations are heading in the same direction.”
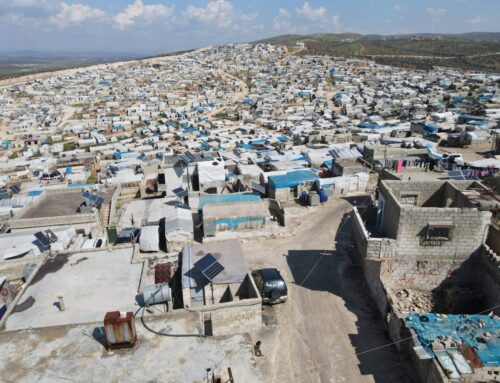
Care is particularly hard to reach for those living in informal camps for internally displaced people. “In the cities you find hospitals, midwives and doctors, but in the camps, women struggle to find dispensaries or medical staff to help them,” Rasha, a 25-year old woman from the city of Homs displaced to Idlib, told Syria Direct. Several NGOs provide primary health services through mobile clinics, but usually refer patients to hospitals for specialized care.
Given the cost of private clinics, most patients prefer to rely on services provided by NGOs. This sometimes means crossing greater distances to seek care, incurring additional costs and risks in a region that is regularly targeted by Russian and regime strikes. For unaccompanied women, who might postpone seeking care rather than face the hassle of traveling alone, this can be particularly challenging, with dramatic consequences. Osama recounted one woman who was recently admitted to an MSF-run emergency room in a state of shock after traveling for days to receive specialized care she urgently needed.
Displacement: the multiplier effect
Health workers in northwestern Syria lament the psychological toll that the war has taken on their female patients, particularly those who are displaced, amidst rising rates of early marriage and pregnancies.
Many displaced women—who often live in informal camps with limited transportation and access to medical services—struggle to access long-term care such as that needed during pregnancy. “Previously, a woman would go to one gynecologist who knew her well, but today she can no longer visit the same doctor because she was displaced, or her doctor left the country,” said Noor Muhammad (a pseudonym), a 30-year old displaced woman from Hama.
Personal investment in routine medical checkup or prenatal care are frequently overridden by the struggles of everyday life. “Women’s interest in their own health has greatly decreased due to the war and the difficulties of life,” Zubaida said. “Women who used to take vitamins and supplements during pregnancy have stopped doing so because they cannot afford them.”
READ MORE: Women in Idlib and the housing crisis
Disruptions in access to family planning services are another unfortunate consequence of the war. In peacetime, women across the world frequently struggle to find contraception methods suited to their needs and bodies. But in Syria, this is compounded by war-induced shortages. “Some contraceptives are no longer available because of the cutting off of crossings between regime areas, where the drug factories are located, and rebel-held areas,” al-Shahoud pointed out.
While some forms of contraception are available overall, women who spoke to Syria Direct complained about their quality and cost, as well as the lack of options. “I use an intrauterine device (IUD) for contraception, but at first the type that I wanted was not available, so I had to use another type known for its negative side effects,” al-Shahoud said.
For the millions of Syrian women who continue to struggle accessing adequate care at all stages of their sexual, reproductive and maternal journey, there is meager hope ahead.
“Before the war, women’s situation was good, their family was by their side,” Rasha added. “Now, she has taken the role of mother, father, brother and sister and is responsible for securing her family’s needs. Women’s health needs, their inability to buy medicine, their double load working inside and outside the home are destroying their health, life and causing increasing psychological problems.”
*Osama and Zubaida requested to be identified by their first names only.